Extending Clinical Visibility Beyond Hospital Walls
Extending Clinical Visibility Beyond Hospital Walls
Extending Clinical Visibility
Beyond Hospital Walls
DischargED.ai brings visibility to one the riskiest phase of care:
post-discharge. We identify recovery deviations early to help you:
Decrease preventable ER revisits
Reduce patient readmissions
Optimize ED throughput
Improve patience experience
All without upsetting existing operational workflows or adding burden to clinical staff.
The Problem
Patient Risk Doesn’t End at Discharge - Recovery Visibility Does
Patient Risk Doesn’t End at Discharge - Recovery Visibility Does
After ER and surgical discharge, patients enter their most vulnerable phase, yet clinical visibility virtually disappears. Existing solutions leave a critical gap:
Traditional RPM is designed for longer-term chronic care with a minimum 16-day window,
missing the immediate post-discharge risks.Telehealth is episodic, providing no virtual telemetry or continuous data to assess real-time recovery pathways.
This disconnect creates unnecessary risk. Without visibility into a patient's progress, early physiological symptoms are missed, allowing patients to deteriorate rapidly:
1 in 3 patients return and require admission within 30 days.
80% of these revisits occur within the first 7 days.
The Result: Worsening patient conditions, increased strain on short-staffed teams, and avoidable costs that burden hospitals at scale.
After ER and surgical discharge, patients enter their most vulnerable phase, yet clinical visibility virtually disappears. Existing solutions leave a critical gap:
Traditional RPM is designed for longer-term chronic care with a minimum 16-day window,
missing the immediate post-discharge risks.Telehealth is episodic, providing no virtual telemetry or continuous data to assess real-time recovery pathways.
This disconnect creates unnecessary risk. Without visibility into a patient's progress, early physiological symptoms are missed, allowing patients to deteriorate rapidly:
1 in 3 patients return and require admission within 30 days.
80% of these revisits occur within the first 7 days.
The Result: Worsening patient conditions, increased strain on short-staffed teams, and avoidable costs that burden hospitals at scale.
We discharge patients every day knowing some will come back. But we have no visibility into how their risk is evolving once they leave.

ER Physician
We keep seeing patients come back, and by then it’s a much bigger problem. That’s where a lot of the cost comes from.

CFO
It’s usually not a sudden event. Something starts to go wrong a few days after discharge. We just don’t see it when it’s happening.

ER Director
Honestly, we are so short-staffed and busy that many patients slip through the cracks. If we had a way to efficiently triage remotely and intervene early, we have a chance at making a real difference.

ER Nurse
We’re still accountable for the outcome, but we lose nearly all visibility the second a patient walks out the door.

Quality Director
We discharge patients every day knowing some will come back. But we have no visibility into how their risk is evolving once they leave.
ER Physician
We keep seeing patients come back, and by then it’s a much bigger problem. That’s where a lot of the cost comes from.
CFO
It’s usually not a sudden event. Something starts to go wrong a few days after discharge. We just don’t see it when it’s happening.
ER Director
Honestly, we are so short-staffed and busy that many patients slip through the cracks. If we had a way to efficiently triage remotely and intervene early, we have a chance at making a real difference.
ER Nurse
We’re still accountable for the outcome, but we lose nearly all visibility the second a patient walks out the door.
Quality Director
We discharge patients every day knowing some will come back. But we have no visibility into how their risk is evolving once they leave.
ER Physician
We keep seeing patients come back, and by then it’s a much bigger problem. That’s where a lot of the cost comes from.
CFO
It’s usually not a sudden event. Something starts to go wrong a few days after discharge. We just don’t see it when it’s happening.
ER Director
Honestly, we are so short-staffed and busy that many patients slip through the cracks. If we had a way to efficiently triage remotely and intervene early, we have a chance at making a real difference.
ER Nurse
We’re still accountable for the outcome, but we lose nearly all visibility the second a patient walks out the door.
Quality Director
The Problem
Patient Risk Doesn’t End at Discharge - Recovery Visibility Does
After ER and surgical discharge, patients enter their most vulnerable phase, yet clinical visibility virtually disappears. Existing solutions leave a critical gap:
Traditional RPM is designed for longer-term chronic care with a minimum 16-day window,
missing the immediate post-discharge risks.Telehealth is episodic, providing no virtual telemetry or continuous data to assess real-time recovery pathways.
This disconnect creates unnecessary risk. Without visibility into a patient's progress, early physiological symptoms are missed, allowing patients to deteriorate rapidly:
1 in 3 patients return and require admission within 30 days.
80% of these revisits occur within the first 7 days.
The Result: Worsening patient conditions, increased strain on short-staffed teams, and avoidable costs that burden hospitals at scale.
We discharge patients every day knowing some will come back. But we have no visibility into how their risk is evolving once they leave.
ER Physician
We keep seeing patients come back, and by then it’s a much bigger problem. That’s where a lot of the cost comes from.
CFO
It’s usually not a sudden event. Something starts to go wrong a few days after discharge. We just don’t see it when it’s happening.
ER Director
Honestly, we are so short-staffed and busy that many patients slip through the cracks. If we had a way to efficiently triage remotely and intervene early, we have a chance at making a real difference.
ER Nurse
We’re still accountable for the outcome, but we lose nearly all visibility the second a patient walks out the door.
Quality Director
We discharge patients every day knowing some will come back. But we have no visibility into how their risk is evolving once they leave.
ER Physician
We keep seeing patients come back, and by then it’s a much bigger problem. That’s where a lot of the cost comes from.
CFO
It’s usually not a sudden event. Something starts to go wrong a few days after discharge. We just don’t see it when it’s happening.
ER Director
Honestly, we are so short-staffed and busy that many patients slip through the cracks. If we had a way to efficiently triage remotely and intervene early, we have a chance at making a real difference.
ER Nurse
We’re still accountable for the outcome, but we lose nearly all visibility the second a patient walks out the door.
Quality Director
Healthcare systems are grappling with this challenge at enormous scale
Healthcare systems
are grappling with this challenge at enormous scale
THE PROBLEM FUNNEL: SIZING THE CRITICAL CARE GAP
THE PROBLEM FUNNEL: SIZING THE CRITICAL
CARE GAP
150M
Emergency Department Visits Each Year
150M
Emergency Department Visits Each Year
125M
“Treat and Release” Patients Annually
50M
Emergency Department
Revisits in <30 Days
18M
Require a First Time
Admission
125M
“Treat and Release”
Patients Annually
50M
Emergency Department
Revisits in <30 Days
18M
Require a First Time
Admission
THE FINANCIAL IMPACT: SIZING THE MARKET
18M
Require a First Time Admission
$10K
Average Direct Operational
Cost per Admission
$180B
Total Financial Problem
for Systems & Payers
Addressing the average direct $10,000 cost per first-time admission across 18 million patients.
The solution
Patient Risk Management After Discharge
Patient Risk Management After Discharge
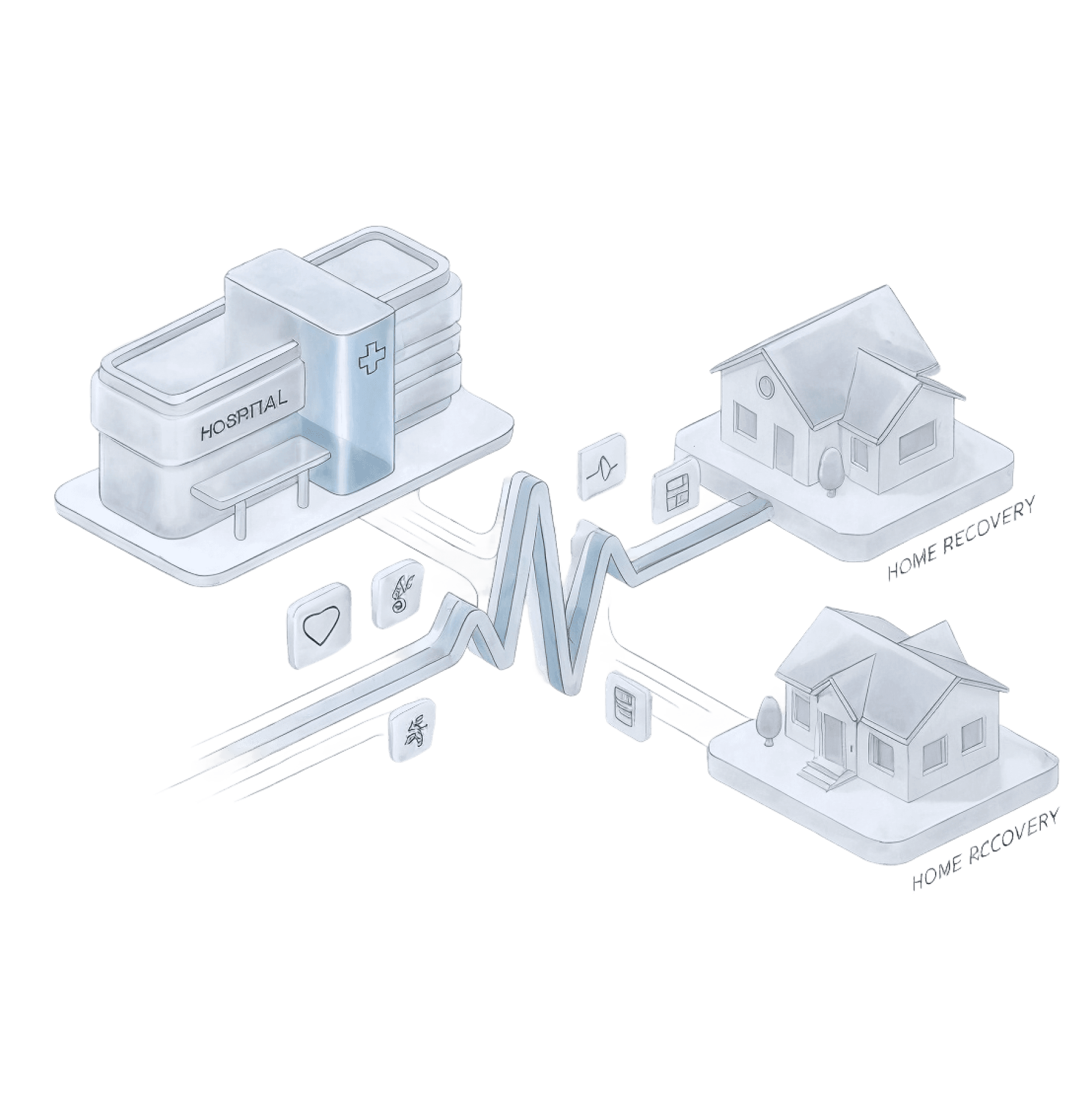
DischargED.ai leverages consumer wearables and AI to monitor patients along their expected recovery pathways, identifying concerning deviations in real time and enabling care teams to intervene before conditions deteriorate.
Zero New Hardware Required: With ~1 in 3 ER patients already using a smartwatch, deployment is immediate.
1. Seamless Connection: Patients connect their existing wearable device before leaving the facility.
2. AI-Assisted Analysis: Physiological signals are continuously analyzed to identify recovery patterns that may require attention.
3. Structured Insights: Clinicians receive clear data to understand if a patient's recovery trajectory is progressing normally.
The platform does not diagnose conditions - it provides clinical visibility where none previously existed.
DischargED.ai leverages consumer wearables and AI to monitor patients along their expected recovery pathways, identifying concerning deviations in real time and enabling care teams to intervene before conditions deteriorate.
Zero New Hardware Required: With ~1 in 3 ER patients already using a smartwatch, deployment is immediate.
1. Seamless Connection: Patients connect their existing wearable device before leaving the facility.
2. AI-Assisted Analysis: Physiological signals are continuously analyzed to identify recovery patterns that may require attention.
3. Structured Insights: Clinicians receive clear data to understand if a patient's recovery trajectory is progressing normally.
The platform does not diagnose conditions - it provides clinical visibility where none previously existed.
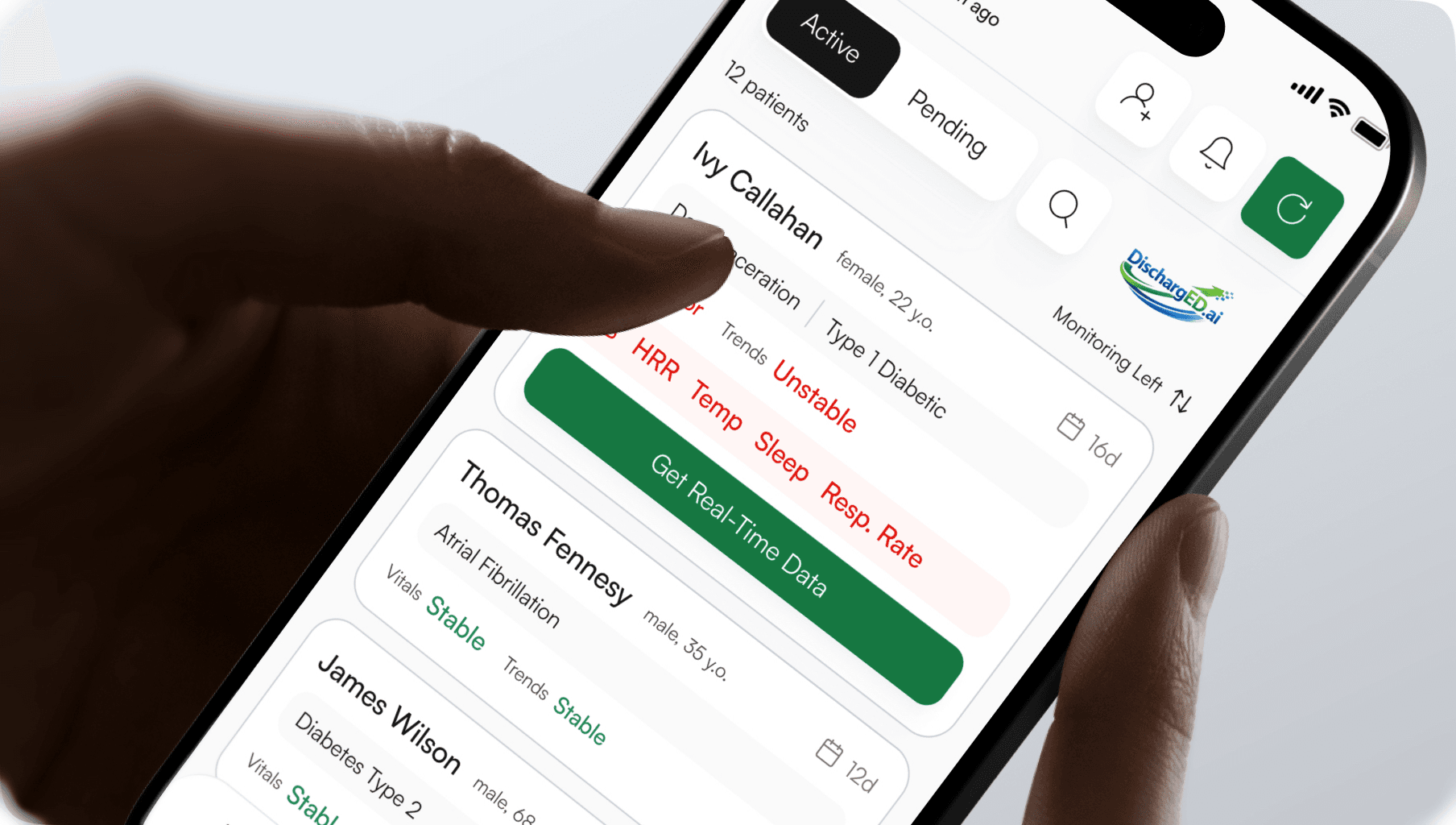
Clinician Command Center
Clinician Command Center
Real-time triage and risk-stratified patient cohorts.
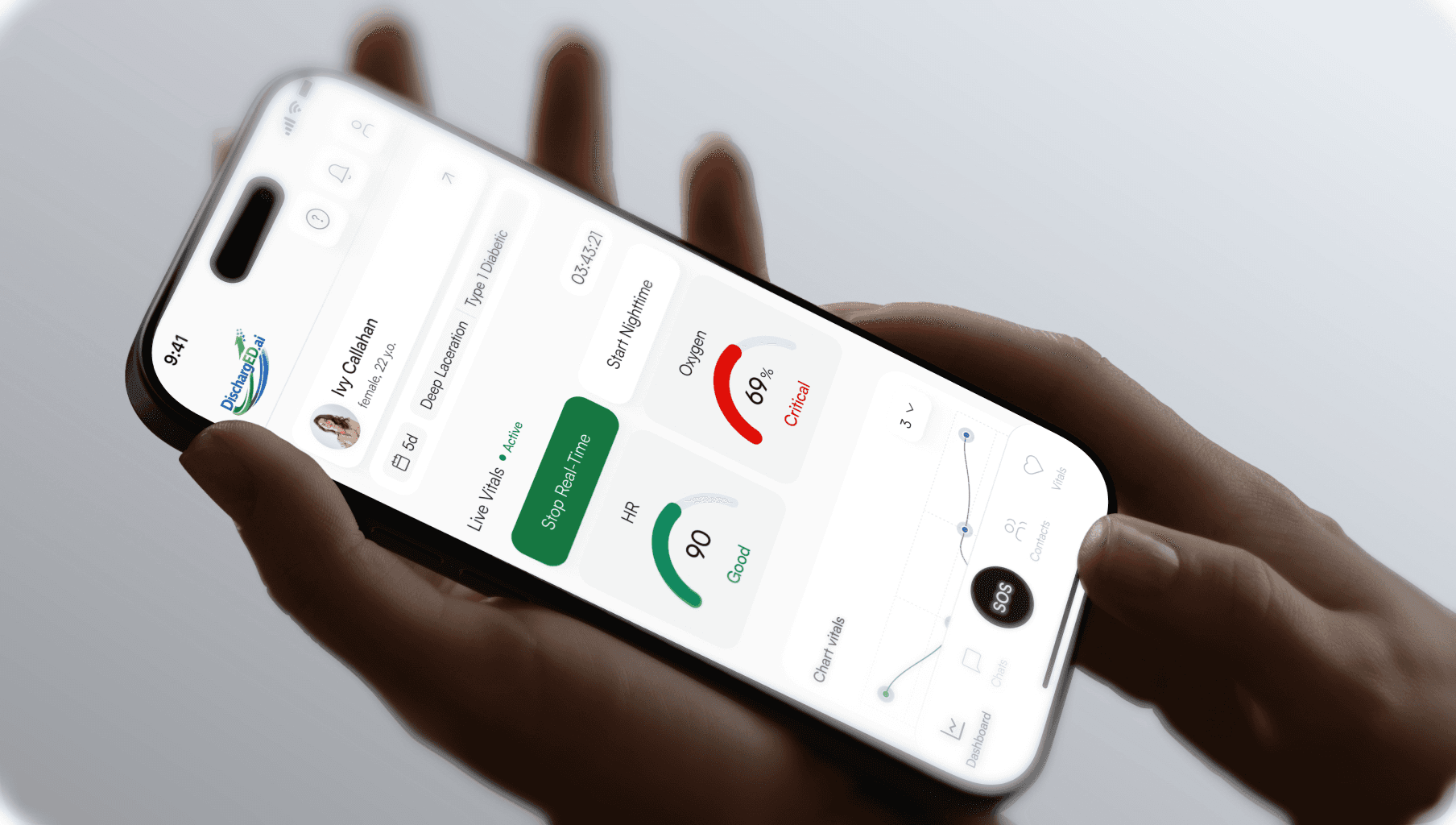
Patient Companion App
Patient Companion App
Frictionless adherence and bio-feedback loops.
Operational Workflow
Operational Workflow
01
Patient Enrollment
Patients connect their smartwatch during discharge. Setup takes just minutes.
Patients connect their smartwatch during discharge. Setup takes just minutes.
02
Recovery Monitoring
Continuous signals from the wearable device provide real-time insight into recovery patterns.
03
Signal Analysis
AI-assisted workflows analyze physiological changes to detect early recovery variances.
AI-assisted workflows analyze physiological changes to detect early recovery variances.
04
Risk Identification
Deviations from expected recovery baselines are immediately flagged
for clinical review.
05
ESCALATION
Care teams receive structured alerts. Clinicians then review the data to determine if intervention is needed.
Physiological Signal Detection
Physiological Signal Detection
Physiological Signal Detection
Clinical-Grade Fidelity
Consumer-Grade Ease
Clinical-Grade Fidelity
Consumer-Grade Ease
Clinical-Grade Fidelity
Consumer-Grade Ease
HRV
HRV
HRV
Continuous BPM monitoring
Continuous BPM monitoring
Continuous BPM monitoring
SpO2
SpO2
SpO2
Oxygen saturation levels
Oxygen saturation
levels
Oxygen saturation levels
Arrhythmia
Arrhythmia
Arrhythmia
Rhythm disturbance alerts
Rhythm disturbance alerts
Rhythm disturbance alerts
Mobility
Mobility
Mobility
Gait and movement analysis
Gait and movement analysis
Gait and movement analysis
Sleep
Sleep
Sleep
Restorative cycle tracking
Restorative cycle tracking
Restorative cycle tracking
Falls
Falls
Falls
Impact & posture analysis
Impact & posture analysis
Impact & posture analysis
BLOOD PRESSURE
BLOOD PRESSURE
BLOOD PRESSURE
Blood pressure trending and alerts
Blood pressure trending and alerts
Blood pressure trending and alerts
TEMPERATURE ANALYSIS
TEMPERATURE ANALYSIS
TEMPERATURE ANALYSIS
Core temperature trending
Core temperature trending
Core temperature trending

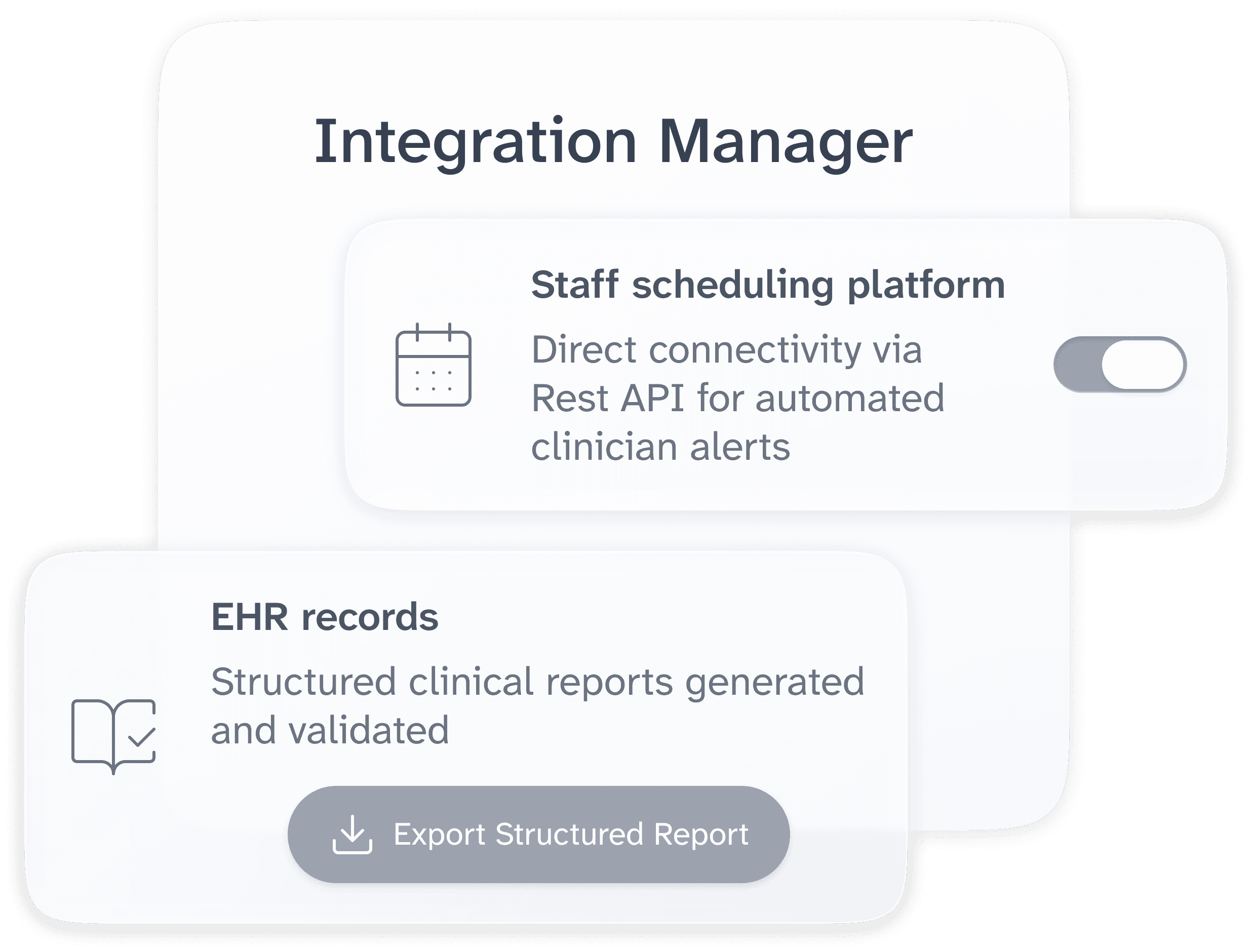
Integration Manager
EHR records
Structured clinical reports generated and validated
Export Structured Report
Staff scheduling platform
Direct connectivity via Rest API for automated clinician alerts
Operational Integration
Operational Integration
Operational
Integration
Deploy quickly. Zero complex IT projects.
DischargED.ai minimizes integration headaches so your facility can launch faster.
No EHR Integration Required
No complex hooks into Epic. Clinicians simply receive structured reports and upload them to EHR only when necessary.
Simple Scheduling Sync
The only integration needed is with your staff scheduling platform (e.g., StaffAdmin) to ensure alerts automatically reach the right clinician on duty.
Deploy quickly. Zero complex IT projects.
DischargED.ai minimizes integration headaches so your facility can launch faster.
No EHR Integration Required
No complex hooks into Epic. Clinicians simply receive structured reports and upload them to EHR only when necessary.
Simple Scheduling Sync
The only integration needed is with your staff scheduling platform (e.g., StaffAdmin) to ensure alerts automatically reach the right clinician on duty.
Bring Post-Discharge Risk Visibility to Your Organisation
Bring Post-Discharge Risk Visibility to Your Organisation
Bring Post-Discharge Risk Visibility to
Your Organisation
Closing the clinical visibility gap.
© 2026 DischargED.ai. All rights reserved.
Closing the clinical visibility gap.
© 2026 DischargED.ai. All rights reserved.
Closing the clinical visibility gap.
© 2026 DischargED.ai. All rights reserved.
Healthcare systems are grappling with this challenge at enormous scale
Healthcare systems are grappling with this challenge at enormous scale
THE PROBLEM FUNNEL: SIZING THE CRITICAL CARE GAP
THE PROBLEM FUNNEL: SIZING THE CRITICAL CARE GAP
150M
150M
Emergency Department Visits Each Year
Emergency Department
Visits Each Year
125M
“Treat and Release” Patients Annually
“Treat and Release”
Patients Annually
50M
Emergency Department
Revisits in <30 Days
Emergency Department
Revisits in <30 Days
18M
Require a First Time
Admission
Require a First Time
Admission
125M
“Treat and Release”
Patients Annually
50M
Emergency Department
Revisits in <30 Days
18M
Require a First Time
Admission
THE FINANCIAL IMPACT: SIZING THE MARKET
18M
Require a First
Time Admission
$10K
Average Direct Operational
Cost per Admission
$180B
Total Financial Problem
for Systems & Payers
Addressing the average direct $10,000 cost per first-time admission across
18 million patients.